
Two medications now dominate the GLP-1 weight loss and diabetes landscape: semaglutide (sold as Ozempic, Wegovy, and Rybelsus) and tirzepatide (sold as Mounjaro and Zepbound). They are often discussed together, prescribed for similar conditions, and confused for one another — yet they are meaningfully different drugs with distinct mechanisms, efficacy profiles, approval statuses, and ideal candidates.
This guide breaks down every major difference between tirzepatide and semaglutide in 2026, drawing on the latest clinical trial data, real-world studies, and updated FDA guidance — so you and your provider can make a genuinely informed decision.
Key takeaways
- Both tirzepatide and semaglutide are once-weekly injectable GLP-1 medications that produce significant weight loss and improve blood sugar control.
- Tirzepatide is a dual GLP-1 + GIP receptor agonist; semaglutide is a GLP-1 agonist only — this is the core mechanistic difference.
- In the definitive SURMOUNT-5 head-to-head trial (NEJM 2025), tirzepatide produced ~20% weight loss vs. ~14% with semaglutide over 72 weeks.
- Side effect profiles are broadly similar; both carry the same FDA boxed warning for thyroid tumors.
- Semaglutide has a longer safety track record, proven cardiovascular benefit data (SELECT trial), and FDA approval for adolescents aged 12+.
- The right choice depends on your goals, health history, insurance, and individual response — not just efficacy averages.
- Consult a Heally licensed provider to determine which medication is right for you.
The core difference between semaglutide and tirzepatide: how each drug works
The most important difference between tirzepatide and semaglutide is their mechanism of action — specifically, which hormone receptors they activate.
Semaglutide
Semaglutide is a GLP-1 (glucagon-like peptide-1) receptor agonist. GLP-1 is a gut hormone released after eating that signals the brain to reduce appetite, slows gastric emptying (so you feel fuller longer), stimulates insulin release from the pancreas, and suppresses glucagon (which would otherwise raise blood sugar). Semaglutide mimics this hormone with a longer half-life, making once-weekly dosing possible.
Ready to start semaglutide treatment? Get a semaglutide prescription online complete a quick medical consultation, and receive medication if approved. Buy semaglutide online and begin your personalized weight loss program with ongoing provider support.
Tirzepatide
Tirzepatide is a dual GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptor agonist — sometimes called a “twincretin.” GIP is a second gut hormone involved in insulin secretion, fat storage regulation, and energy metabolism. By activating GIP receptors alongside GLP-1 receptors simultaneously, tirzepatide creates synergistic metabolic effects that exceed what either hormone achieves alone. Critically, GIP receptor activation in adipose (fat) tissue appears to enhance fat mobilization and energy expenditure beyond what GLP-1 can do alone — which helps explain tirzepatide’s superior weight loss outcomes in clinical trials.
Ready to start tirzepatide treatment? Get a tirzepatide prescription online complete a medical consultation, and receive medication if approved. Buy tirzepatide online and begin your personalized weight loss treatment with ongoing provider support.
Mechanism edge: tirzepatide
Tirzepatide’s dual GLP-1 + GIP action creates broader metabolic benefits. However, both mechanisms are clinically proven — semaglutide’s GLP-1-only approach produces substantial, well-documented weight loss and glycemic control in its own right.
FDA approvals: what each drug is officially indicated for
| Indication | Semaglutide | Tirzepatide |
| Type 2 diabetes management | Ozempic (injectable), Rybelsus (oral) | Mounjaro |
| Chronic weight management (obesity) | Wegovy (adults + adolescents 12+) | Zepbound (adults only) |
| Cardiovascular risk reduction (ASCVD) | Wegovy (SELECT trial, 2023) | Studies ongoing (SURPASS-CVOT) |
| Obstructive sleep apnea (OSA) | Not approved | Zepbound (approved 2024) |
| Use in adolescents (12–17 years) | Wegovy (12+ years, obesity) | Not approved under 18 |
| Oral formulation available | Rybelsus (oral tablets, T2D) | Injectable only |
| Metabolic dysfunction-associated steatohepatitis (MASH) | Wegovy HD (approved 2025) | Not yet approved |
Sources: FDA prescribing information for Wegovy (2025), Mounjaro (2026), Zepbound (2025); FDA Wegovy label 2025; FDA Mounjaro label 2026
Approvals breadth edge: semaglutide
Semaglutide currently holds more FDA indications — including proven cardiovascular benefit, adolescent use, an oral formulation, and the newly approved MASH indication — giving it an advantage in breadth of clinical application.
Semaglutide and tirzepatide efficacy in weight loss comparison
This is where the two drugs diverge most clearly, and where the most robust clinical evidence now exists.
| Drug | Trial | Duration | Dosage | Mean Weight Reduction |
| Tirzepatide | SURMOUNT-5 | 72 weeks | — | −20.2% |
| Semaglutide | SURMOUNT-5 | 72 weeks | — | −13.7% |
| Tirzepatide | SURMOUNT-1 | 72 weeks | 15 mg | −22.5% |
| Semaglutide | STEP-1 | 68 weeks | 2.4 mg | −14.9% |
The SURMOUNT-5 trial — published in the New England Journal of Medicine in May 2025 — was the first randomized, head-to-head comparison of the two medications in patients with obesity but without type 2 diabetes. It enrolled 751 adults and ran for 72 weeks at the maximum tolerated dose of each drug. Tirzepatide produced a mean weight reduction of 20.2% compared to 13.7% with semaglutide — a statistically significant 6.5 percentage point difference. Participants on tirzepatide were also more likely to achieve weight reductions of 10%, 15%, 20%, and 25% compared to those on semaglutide.
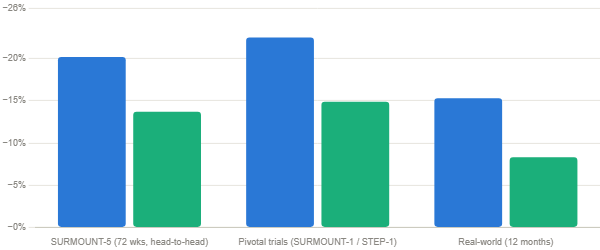
A 2025 meta-analysis in PMC (covering 36,754 tirzepatide and 106,057 semaglutide participants across multiple studies) confirmed tirzepatide’s advantage, finding an average 4.23 percentage points greater weight loss with tirzepatide — an effect that was both dose- and duration-dependent. Real-world data from a large U.S. study of over 18,000 patients found tirzepatide users lost approximately 15.3% of body weight at 12 months compared to 8.3% with semaglutide.
Weight loss edge: tirzepatide
The clinical evidence is now definitive — tirzepatide produces greater average weight loss than semaglutide across trials and real-world data. That said, semaglutide still produces clinically meaningful, life-improving weight loss for the majority of patients.
Semaglutide and tirzepatide efficacy in blood sugar control for type 2 diabetes
Both medications significantly reduce HbA1c (the key long-term blood sugar marker), but tirzepatide again shows superior results in head-to-head comparisons.
| Metric | Tirzepatide | Semaglutide |
| HbA1c reduction (max dose, trials) | −2.0% to −2.4% | −1.6% to −1.9% |
| HbA1c reduction (real-world, 12 mo) | −1.3% (GLP-1 naïve patients) | −0.9% (GLP-1 naïve patients) |
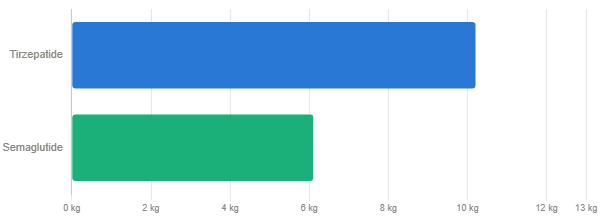
| Weight lost (real-world, T2D, 12 mo) | −10.2 kg | −6.1 kg |
| SURPASS-2 vs. 1 mg sema (HbA1c) | −2.0 to −2.3% (all tirzepatide doses) | −1.86% (1 mg weekly) |
| Cardiovascular outcomes (MACE) | Data pending (SURPASS-CVOT) | Proven reduction (SELECT trial) |
Sources: Real-world HbA1c study, PMC 2025; SURPASS-2, NEJM 2021
An important caveat: semaglutide’s proven cardiovascular benefit is a meaningful clinical differentiator. The SELECT trial (2023) demonstrated that Wegovy significantly reduces major adverse cardiovascular events (MACE) — heart attack, stroke, cardiovascular death — in patients with established cardiovascular disease and obesity. Tirzepatide’s cardiovascular outcomes trial (SURPASS-CVOT) is still ongoing as of 2026. For patients with a history of heart disease, this proven benefit may tip the clinical balance toward semaglutide.
2026 Update. In 2025, the FDA approved Wegovy HD — a higher-dose semaglutide formulation — for metabolic dysfunction-associated steatohepatitis (MASH), formerly known as NASH. This expanded semaglutide’s clinical reach significantly. Additionally, Zepbound (tirzepatide) received approval for obstructive sleep apnea (OSA) in adults with obesity in 2024, marking the first FDA-approved pharmacotherapy for OSA.
Semaglutide and tirzepatide dosing comparison
| Dosing Feature | Semaglutide | Tirzepatide |
| Starting dose | 0.25 mg weekly (injectable) / 3 mg daily (oral) | 2.5 mg weekly |
| Titration interval | Every 4 weeks | Every 4 weeks |
| Maintenance dose range | 0.5 mg – 2.4 mg weekly (injectable) | 5 mg – 15 mg weekly |
| Maximum dose | 2.4 mg weekly (Wegovy) / 2 mg weekly (Ozempic) | 15 mg weekly |
| Administration | Subcutaneous injection or oral tablet (Rybelsus) | Subcutaneous injection only |
| Injection device | Pre-filled auto-injector pen | Pre-filled auto-injector pen |
| Half-life | ~7 days | ~5 days |
Semaglutide and tirzepatide side effects: how do they compare?
Because both drugs activate the GLP-1 pathway, their side effect profiles are substantially similar. The differences are matters of degree rather than kind.
Common side effects shared by both medications:
- Nausea (most common, usually transient — peaks during dose escalation)
- Vomiting
- Diarrhea or constipation
- Decreased appetite and early satiety
- Bloating or stomach discomfort
- Injection site reactions
Key safety warnings that apply to both drugs:
- FDA Boxed Warning (both): Possible risk of thyroid C-cell tumors, based on animal studies. Both are contraindicated in patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
- Pancreatitis risk — both carry a warning; discontinue if suspected.
- Gallbladder disease — both associated with increased gallstone and cholecystitis risk, particularly with rapid weight loss.
- Hypoglycemia — especially in patients with type 2 diabetes who are also taking insulin or sulfonylureas.
- Renal impairment — both can worsen dehydration-related acute kidney injury if GI side effects are severe.
Where do they differ in side effects?
A meta-analysis covering over 28,000 patients found that while the overall rate of GI adverse events was similar (approximately 52–53% of patients in both groups), serious adverse events occurred somewhat more frequently with higher tirzepatide doses (5.3–7% at 10–15 mg) compared to semaglutide (2.8%). Appetite suppression can also be more pronounced on tirzepatide, which some patients welcome but others find uncomfortable.
Side effect tolerability edge: semaglutide (slight)
Both drugs have similar side effect profiles overall. Semaglutide has a slightly better serious adverse event rate in comparative data, and its GLP-1-only mechanism tends to produce somewhat less pronounced appetite suppression. Semaglutide also benefits from a longer real-world safety track record (approved for weight loss since 2021).
Semaglutide and tirzepatide difference in cost and insurance in 2026
Cost is often the deciding factor for many patients. Brand-name versions of both medications are expensive without insurance, but the landscape has shifted considerably in 2026.
| Cost factor | Semaglutide | Tirzepatide |
| Brand-name monthly cost (list price) | ~$1,000–$1,350 (Wegovy/Ozempic) | ~$1,050–$1,500 (Mounjaro/Zepbound) |
| Insurance coverage (obesity) | Broader — Wegovy has longer formulary history | Growing — Zepbound gaining coverage |
| Manufacturer savings card | Novo Nordisk savings program available | Eli Lilly savings card available |
| Compounded availability (2026) | Variable — FDA shortage status fluctuates | Available through licensed pharmacies |
| Cost per 1% body weight reduction | ~$1,845 (brand-name) | ~$985 (brand-name) |
Note: Compounded GLP-1 options through licensed pharmacies can reduce costs significantly. Prices as reported in 2026; confirm current pricing with your pharmacy or provider. Source: Drugs.com comparison, updated March 2026
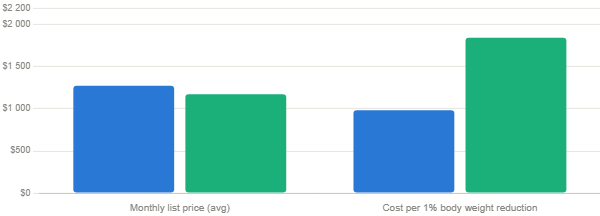
Despite similar list prices, tirzepatide’s greater weight loss makes it nearly 2× more cost-efficient per unit of outcome. Source: Drugs.com, March 2026.
When measured in cost per percentage point of body weight lost, tirzepatide is actually more cost-efficient than semaglutide at brand-name prices, despite its similar or slightly higher list price — because it produces greater weight loss per dollar spent.
Who should choose tirzepatide?
- Patients whose primary goal is maximum weight loss and who want the drug with the strongest efficacy data
- Those who have plateaued on semaglutide and need a more potent treatment
- Adults with obesity and obstructive sleep apnea (the only FDA-approved pharmacotherapy for OSA)
- Type 2 diabetes patients who need stronger HbA1c reduction beyond what semaglutide can provide
- Patients for whom insurance covers tirzepatide at comparable or lower cost to semaglutide
Who should choose semaglutide?
- Patients with established cardiovascular disease (heart attack, stroke history) who benefit from semaglutide’s proven MACE reduction (SELECT trial)
- Adolescents aged 12–17 with obesity — Wegovy is the only approved GLP-1 option in this age group
- Patients who prefer or need an oral medication option (Rybelsus tablets for type 2 diabetes)
- Those for whom semaglutide is more affordable or better covered by insurance
- Patients with metabolic dysfunction-associated steatohepatitis (MASH) — Wegovy HD received approval for this indication in 2025
- First-time GLP-1 users who want to start with the medication with the longest real-world safety track record
Frequently Asked Questions
Is tirzepatide stronger than semaglutide?
In terms of average weight loss and blood sugar reduction in clinical trials, yes — tirzepatide consistently outperforms semaglutide. The SURMOUNT-5 head-to-head trial confirmed tirzepatide produced about 20% weight loss vs. about 14% with semaglutide over 72 weeks. However, “stronger” doesn’t mean “right for everyone.” Individual responses vary significantly, and semaglutide produces clinically meaningful results for the majority of patients who take it.
Can I take tirzepatide and semaglutide together?
No. These medications should never be taken simultaneously. Both act on GLP-1 receptors, and combining them greatly increases the risk of severe GI side effects, hypoglycemia (in diabetes patients), and other adverse events, without providing additional clinical benefit. Always complete one medication cycle before starting the other, with your provider’s guidance.
Which is better for weight loss: Ozempic or Mounjaro?
Mounjaro (tirzepatide) produces greater average weight loss than Ozempic (semaglutide) in clinical trials. However, note that Ozempic is technically approved for type 2 diabetes, not obesity — Wegovy is the weight-loss-approved form of semaglutide. For a direct comparison see our pages on Ozempic and Mounjaro. For obesity treatment, the relevant comparison is Zepbound vs. Wegovy.
Which drug has fewer side effects?
Both medications have broadly similar side effect profiles dominated by GI symptoms — nausea, vomiting, diarrhea, and constipation. Comparative data shows slightly higher rates of serious adverse events with high-dose tirzepatide (10–15 mg). If you had intolerable side effects on one medication, switching to the other under medical supervision may improve tolerability, since the molecules are different enough to produce different individual responses.
Does semaglutide have better cardiovascular benefits than tirzepatide?
Currently, yes — semaglutide has proven cardiovascular benefit from the SELECT trial (2023), which demonstrated significant reduction in major adverse cardiovascular events (heart attack, stroke, cardiovascular death) in patients with obesity and established heart disease. Tirzepatide’s cardiovascular outcomes trial (SURPASS-CVOT) is ongoing as of 2026, so this comparison may change once those results are published.
Which is more cost-effective?
Despite similar or slightly higher list prices, tirzepatide’s greater weight loss per patient makes it more cost-efficient per percentage point of body weight lost — approximately $985 vs. $1,845 per 1% weight reduction at brand-name prices. However, out-of-pocket cost depends heavily on your insurance coverage, which varies between patients and plans. Always check your specific formulary before deciding based on cost.
Is there a generic version of either drug available?
No FDA-approved generics exist for either tirzepatide or semaglutide as of April 2026. Both are still under patent protection. Compounded semaglutide and tirzepatide — prepared by licensed compounding pharmacies using pharmaceutical-grade active ingredients — have provided cost-effective alternatives for many patients, though their availability fluctuates with FDA shortage determinations. Discuss compounded options with your Heally provider.
Resources & further reading
- SURMOUNT-5: Tirzepatide vs. Semaglutide for Obesity (NEJM, 2025)
- Rodriguez et al. — Semaglutide vs. Tirzepatide for Weight Loss (JAMA Internal Medicine, 2024)
- Meta-analysis: Comparative Efficacy of Tirzepatide vs. Semaglutide (PMC, 2025)
- Real-world HbA1c and weight outcomes: Tirzepatide vs. Semaglutide in T2D (PMC, 2025)
- SURPASS-2: Tirzepatide vs. Semaglutide in Type 2 Diabetes (NEJM, 2021)
Medical disclaimer
This article is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment. The information provided reflects publicly available clinical data and general guidance as of April 2026. Clinical trial results represent population averages and individual responses to any medication will vary. Both semaglutide and tirzepatide are prescription medications requiring a licensed healthcare provider’s evaluation and prescription. Do not start, stop, or change any medication without consulting your doctor. Heally connects patients with independent licensed healthcare providers; Heally itself does not prescribe medications or provide medical advice. All pricing information is approximate and subject to change; verify costs with your pharmacy and insurance carrier.
